Devices & Supplies
Some routes of administration demand that products do not bring microbial contamination with them into the body. This is required because some routes of administration by-pass the body’s natural defense mechanisms, or some tissues or organs are so sensitive and vital that such contamination could be serious.
All of these “sterility demanding” routes are parenteral routes.
NOTE: But not all parenteral routes are “sterility demanding” routes.
 The term parenteral means next to or beside the enteral. Enteral refers to the alimentary tract, so parenteral means sites that are outside of or beside the alimentary tract. Since oral, sublingual, and rectal comprise the enteral routes of administration, any other route is considered a parenteral administration site. Topical administration is a parenteral route that does not require sterile formulations.
The term parenteral means next to or beside the enteral. Enteral refers to the alimentary tract, so parenteral means sites that are outside of or beside the alimentary tract. Since oral, sublingual, and rectal comprise the enteral routes of administration, any other route is considered a parenteral administration site. Topical administration is a parenteral route that does not require sterile formulations.
The parenteral routes of administration are used for various reasons.
- If a drug is poorly absorbed when orally administered or is degraded by stomach acid or the gastrointestinal enzymes, then a parenteral route would be indicated.
- The parenteral routes are also preferred when a rapid and predictable drug response is desired as in a emergency situation.
- Parenteral routes of administration are also useful when a patient is uncooperative, unconscious, or unable to take drug via an enteral route.
- Parenteral routes are used when localized drug therapy is desired.
But there are major disadvantages.
- Most of these parenteral formulations are more expensive than enteral route formulations.
- There is the requirement that these parenteral formulations must be sterile.
- Most of these formulations require that a skilled or trained person administer them.
- Once the drug is administered, it may be difficult to remove the dose is there if an adverse or toxic reaction.
Large Volume Parenteral (LVP) Solutions
Parenteral solutions are packaged as large volume parenteral (LVP) solutions and small volume parenteral (SVP) solutions. LVP solutions are typically bags or bottles containing larger volumes of intravenous solutions. Common uses of LVP solutions without additives include: 1) correction of electrolyte and fluid balance disturbances; 2) nutrition; and 3) vehicle for administering other drugs.
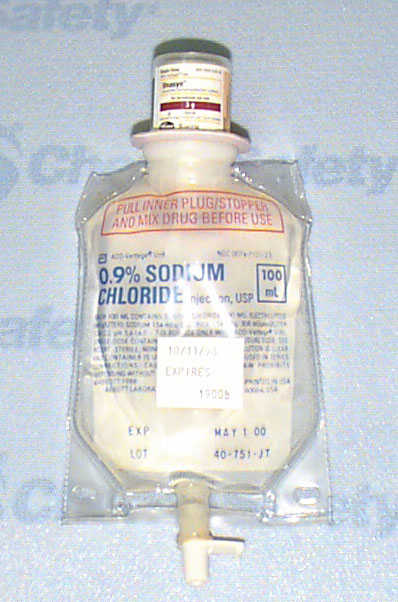
Large volume parenteral solutions are packaged in containers holding 100 ml or more. There are three types of containers: glass bottle with an air vent tube, glass bottle without an air vent tube, and plastic bags.
Plastic bags have advantages over glass bottles: they do not break; they weigh less; they take up less storage space, and they take up much less disposal space. However, some drugs adsorb to the plastic. Also, some drugs and solutions leach a plasticizer out of the plastic; the plasticizer is included to keep the plastic pliable. There are now newer plastics that minimize some of these problems.
Plastic bags are available in different sizes. The most common sizes are 250, 500, and 1,000 ml. The top of the bag has a flap with a hole in it to hang the bag on an administration pole. Graduation marks are on the front of the bag to indicate the volume of solution used. They are marked at 25 ml to 100 ml intervals depending on the overall size of the bag. The plastic bag system collapses as the solution is administered so a vacuum is not created inside the bag.
At one end of the bag are two ports of about the same length. One is the administration set port and the other is the medication port. The administration set port has a plastic cover on it to maintain the sterility of the bag; the cover is easily removed. Solution will not drip out of the bag through this port because of a plastic diaphragm about ½ inch inside the port. When the spike of the administration set is inserted into the port, the diaphragm is punctured, and the solution will flow out of the bag into the administration set. This inner diaphragm cannot be resealed once it is punctured. The medication port is also covered by a protective rubber tip. Drugs are added to the solution through this port using a needle and syringe. There is an inner plastic diaphragm about ½ inch inside the port, just like the administration set port. This inner diaphragm is also not self-sealing when punctured by a needle, but the protective rubber tip prevents solutions from leaking from the bag once the diaphragm is punctured.
Because of the advantages of plastic bags, glass LVP solution bottles are not often used. The major advantage of glass bottles is to administer drugs that are incompatible with plastic bags. Glass intravenous bottles are packaged with a vacuum, sealed with a solid rubber closure, and the closure is held in place by an aluminum band. Graduation marks are along the sides of the bottle and are usually spaced every 20 ml to 50 ml. The solution bottle is hung on an administration pole in an inverted position using the aluminum or plastic band on the bottom of the bottle.
Solutions in either the plastic bag or glass bottle flow from the containers to the patient through an administration set. But for solutions to flow out of a glass container, air must be able to enter the container to relieve the vacuum as the solution leaves. Some bottles have air tubes built into the rubber closure for this purpose. Some bottles do not, in which case an administration set with a filtered airway in the spike must be used.
Many different LVP solutions are commercially available. Four solutions are commonly used either as primary fluids (infused at 2 – 3 ml per minute) or as the base of an admixture solution. The solutions are sodium chloride solution, dextrose solution, Ringer’s solution, and Lactated Ringer’s solution. Various combinations of different strengths of sodium chloride and dextrose solutions are also available, i.e., 5% dextrose and 0.45% sodium chloride, or 5% dextrose and 0.2% sodium chloride.
Small Volume Parenteral Solutions
Small volume parenteral (SVP) solutions are usually 100 ml or less and are packaged in different ways depending on the intended use. If the SVP is a liquid that is used primarily to deliver medications, it is packaged in a small plastic bag called a minibag of 50 – 100 ml (minibags look like small plastic LVP bags). SVPs can also be packaged as ampules, vials, and prefilled syringes. Liquid drugs are supplied in prefilled syringes, heat-sealed ampules, or in vials sealed with a rubber closure. Powdered drugs are supplied in vials and must be constituted (dissolved in a suitable liquid) before being added to any solution. SVPs packaged as ampules, vials, or prefilled syringes are typically added to a minibag or a LVP but they may also serve as the final container. The term admixture is used to denote a solution where such an additive has been added to a minibag or LVP.
Ampules are sealed glass containers with an elongated neck that must be broken off. Most ampules are weakened around  the neck for easy breaking; these will have a colored band around the neck. If the ampule is not weakened, it must first be scored with a file; otherwise the top may shatter. A 5 micron filter needle should be used when drawing the contents of an ampule into a syringe since glass particles may have fallen inside the ampule when the top was snapped off. The filter needle should be removed and replaced with the regular needle before injecting the drug into any solution. In addition, it is useful to wrap an alcohol wipe or small piece of gauze around the top of the ampule before breaking it. This will provide some protection to the fingers if the ampule shatters and will also reduce the possibility of glass splinters becoming airborne.
the neck for easy breaking; these will have a colored band around the neck. If the ampule is not weakened, it must first be scored with a file; otherwise the top may shatter. A 5 micron filter needle should be used when drawing the contents of an ampule into a syringe since glass particles may have fallen inside the ampule when the top was snapped off. The filter needle should be removed and replaced with the regular needle before injecting the drug into any solution. In addition, it is useful to wrap an alcohol wipe or small piece of gauze around the top of the ampule before breaking it. This will provide some protection to the fingers if the ampule shatters and will also reduce the possibility of glass splinters becoming airborne.
Drugs and other additives are packaged in vials either as liquids or lyophilized powders. Vials are made of glass or plastic  and are sealed with a rubber stopper. A needle is used to add contents to or withdraw contents from the vial. Before withdrawing contents from a vial, an equal volume of air is usually injected into the vial to pressurize the vial and aid in withdrawing the contents. However, some medications are packaged under pressure or may produce gas (and therefore pressure) upon reconstitution. In these situations, air should not be injected into the vial before withdrawing the solution.
and are sealed with a rubber stopper. A needle is used to add contents to or withdraw contents from the vial. Before withdrawing contents from a vial, an equal volume of air is usually injected into the vial to pressurize the vial and aid in withdrawing the contents. However, some medications are packaged under pressure or may produce gas (and therefore pressure) upon reconstitution. In these situations, air should not be injected into the vial before withdrawing the solution.
Dry powder formulations are lyophilized or freeze-dried powders that must be reconstituted with some suitable solvent to make a liquid formulation before being withdrawn from the vial. Some drugs are not stable in liquid form and so these drugs are put into the powder form and reconstituted just prior to use. There are several solvents that might be used to reconstitute the dry powders; the appropriate solvent is indicated in the product information insert. The most common solvents are Sterile Water for Injection, Bacteriostatic Water for Injection, Sodium Chloride Injection, and Ringer’s Injection.
 Vials may be designated for single-dose or multi-dose use. Single-dose vials do not contain preservatives and should be discarded after one use. Multidose vials contain a preservative to inhibit bacterial contamination once the vial has been used. Also, the rubber closure will reseal on a multidose vial. This provides a vial from which a number of doses of variable volume can be withdrawn.
Vials may be designated for single-dose or multi-dose use. Single-dose vials do not contain preservatives and should be discarded after one use. Multidose vials contain a preservative to inhibit bacterial contamination once the vial has been used. Also, the rubber closure will reseal on a multidose vial. This provides a vial from which a number of doses of variable volume can be withdrawn.
There are two varieties of prefilled syringes. One type, a cartridge type package, is a single syringe and needle unit which is to be placed in a special holder before use. Once the syringe and needle unit is used, they are discarded but the holder is used again with a new unit. The other type of prefilled syringe consists of a glass tube closed at both ends with rubber stoppers. The prefilled tube is placed into a specially designed syringe that has a needle attached to it. After using this type or prefilled syringe, all of the pieces are discarded.
 Ready-to-mix systems consist of a specially designed minibag with an adapter for attaching a drug vial. The admixing
Ready-to-mix systems consist of a specially designed minibag with an adapter for attaching a drug vial. The admixing  takes place just prior to administration. The major advantages of ready-to-mix systems include a significant reduction in waste and lower potential for medication error because the drug vial remains attached to the minibag and can be rechecked as needed. However, the systems do cost more, and there is the potential that the system will not be properly activated so that the patient receives only the diluent or a partial dose of drug.
takes place just prior to administration. The major advantages of ready-to-mix systems include a significant reduction in waste and lower potential for medication error because the drug vial remains attached to the minibag and can be rechecked as needed. However, the systems do cost more, and there is the potential that the system will not be properly activated so that the patient receives only the diluent or a partial dose of drug.
Filtration and Filters
Filtration is used to remove particles from solutions. These particles might be particulate matter or they may be microorganisms. Filtration is not a “terminal sterilization” procedure as are steam (moist heat), dry heat, ionized radiation, or gas sterilization. Filtration will sterilize the product, but after filtration, the sterile product is then aseptically combined with its packaging. Filtration is used for materials that are chemically or physically unstable if sterilized by heat, gas, or radiation.
There are two types of filters, depth filters and membrane filters.
Depth filters are seldom used for sterilization. They are constructed of randomly oriented fibers or particles (e.g., diatomaceous earth, porcelain, asbestos) that have been pressed, wound, or otherwise bonded together to form a tortuous pathway for flow. The microorganisms are either entrapped in the path or adsorbed to the filter material. The random structure of material inside the filter creates fluid flow pathways that can vary from extremely narrow to very wide. Filter materials can also break off or come loose during filtration and appear in the filtrate.
Depth filters are rigid enough to filter a solution being pulled into a syringe. They can also be used to filter a solution being pushed out of a syringe. But the same filter cannot be used to draw up and then expel a solution. A new needle is required before pushing the solution out of the syringe. If the solution is expelled through the original filter needle, the solution will be re-contaminated.
 Screen filters have a continuous uniform structure that consists of fixed size pores. Particles that are larger than the pore openings cannot pass through the filter and are retained on the surface of the filter. The amount of material retained by a screen filter is limited by the surface area of the filter. Screen filter pore sizes can be predetermined and precisely controlled during manufacturing.
Screen filters have a continuous uniform structure that consists of fixed size pores. Particles that are larger than the pore openings cannot pass through the filter and are retained on the surface of the filter. The amount of material retained by a screen filter is limited by the surface area of the filter. Screen filter pore sizes can be predetermined and precisely controlled during manufacturing.
View a video demonstration on how to use filters on syringes
The most common screen filter used in compounding is called a “membrane filter.” In terms of structure, membrane filters are thin microporous sheets made from a variety of plastics. Membrane filters must have a nominal pore size of 0.22 microns or less if they are to be used for sterilization. However, membrane filters are available in a wide range of pore sizes from 0.11 to 10 microns.
Membrane filters are intended to filter a solution only as it is expelled from a syringe. If a solution is to be drawn into a syringe and then filtered through a membrane filter, use the following procedure:
- A regular needle (or a depth filter needle) is attached to the syringe.
- The solution is pulled into the syringe.
- Air bubbles are removed from the syringe.
- The needle is removed from the syringe.
- A membrane filter unit is then attached to the syringe.
- A regular needle is placed on the needle end of the filter.
- Air is eliminated from the filter chamber by holding the syringe in a vertical position so that the needle is pointing upward. Air must be expelled before the filter becomes wet; otherwise, the air will not pass through the filter.
- Once air has been expelled, pressure should be slowly and continuously applied to push the solutions through the filter.
Membrane filters also eliminate the risk of air embolism. Once a membrane filter is wet, air cannot pass through it unless the “bubble point pressure” of the filter is exceeded. “Bubble point pressure” for a 0.22 micron membrane filter is approximately 55 psi, a pressure that will not occur during parenteral administration. So any air that enters the administration set will be stopped at the filter surface and not allowed to enter the patient’s body.
The same bubble point pressure is used in another way. After a filter is used, the integrity of the filter can be determined if the wetted filter is exposed to a high pressure. If the filter is intact, the appearance of bubbles on the filter surface should occur when the pressure is about 50 – 55 psi. However, if the filter integrity has been compromised, the bubble point pressure will be much lower.
 Membrane filters are often packaged in a round plastic holder which can easily be attached to the end of syringes. Some filters are attached to administration sets and serve as “final filters” and filter the solution immediately before it enter the patient’s vein. Some administration sets have filters already built into the set. Filters can also be placed inside of needles; these are called “filter needles.” There
Membrane filters are often packaged in a round plastic holder which can easily be attached to the end of syringes. Some filters are attached to administration sets and serve as “final filters” and filter the solution immediately before it enter the patient’s vein. Some administration sets have filters already built into the set. Filters can also be placed inside of needles; these are called “filter needles.” There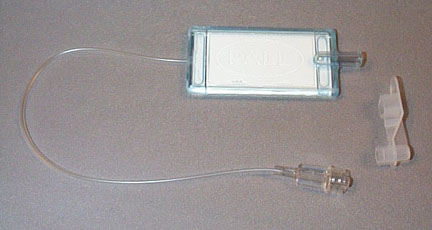 are double ended filter needles which is a simple unit that has a filter between two needles. This allows solution transfer directly from one container to another container and eliminates the need of using a syringe to transfer the solution. Filters are also supplied as single membrane units to be used in specialized filtration apparatus.
are double ended filter needles which is a simple unit that has a filter between two needles. This allows solution transfer directly from one container to another container and eliminates the need of using a syringe to transfer the solution. Filters are also supplied as single membrane units to be used in specialized filtration apparatus.
Several things must be considered when selecting a membrane filter. Hydrophilic filters are easily wetted and are used for aqueous solutions. Hydrophobic filters repel water but allow solvents such as alcohol and air to pass. So these filters would be used to sterilize solutions containing alcohol or isopropyl alcohol, or as air filters. Other considerations include the volume capacity of the filter, how much pressure can be applied to the filter without damaging its integrity, and what is the filter’s compatibility or adsorption profile for the material being filtered.
The material to be filtered also requires some considerations. Viscous oils can be filtered, but it is a time consuming process. Heating the oil will reduce its viscosity and make filtration easier. Some powders can also be filtration sterilized by first dissolving the powder in a solvent, filtering the resultant solution, and then evaporating the solvent under aseptic conditions.
Consideration must also be given to the sterilization of containers, closures, and apparatus. A non-sterile surface that comes in contact with a sterilized product will render the product non-sterile. These contact surfaces must also be pyrogen free. The temperatures and times necessary for depyrogenation are substantially greater than those for sterility. It will probably be necessary to depyrogenate containers, closures, and apparatus separately from the formulation and then aseptically combine them.
Administration Devices
Administration Set
.jpg) The basic method to administer a LVP solution is to use an administration set. The set contains a spiked plastic device to pierce a port on the IV container. This connects to a sight or drip chamber that may be used to set the flow rate, the rate ordered by the physician at which the solution is to be administered to the patient (generally measured in ml/hour). A clamp pinching the tubing also regulates flow. The line then leads to a rubber injection port to which a needle may be attached or to an infusion pump which will control the flow rate.
The basic method to administer a LVP solution is to use an administration set. The set contains a spiked plastic device to pierce a port on the IV container. This connects to a sight or drip chamber that may be used to set the flow rate, the rate ordered by the physician at which the solution is to be administered to the patient (generally measured in ml/hour). A clamp pinching the tubing also regulates flow. The line then leads to a rubber injection port to which a needle may be attached or to an infusion pump which will control the flow rate.
Heparin Lock
In some instances, a patient may not have a primary LVP solution, yet must receive piggyback medications. This is done through a heparin lock, which is a short piece of tubing attached to a needle or intravenous catheter. When the tubing is not being used for the piggyback, heparin is used to fill the tubing. This drug prevents blood from clotting in the tube.
Other Devices
Infusion pumps, syringe pumps, and ambulatory pumps are devices used to administer LVP solutions and control flow rates. Administration sets are threaded through infusion pumps, and the pumps control gravity flow. Syringe pumps expel solutions from a syringe into an administration set such as a heparin lock. An ambulatory pump is about the size of a hand. It allows patients to have some freedom of movement compared to being restricted to an infusion pump attached to an administration pole. Infusion pumps have made the infusion process much more accurate and easier to administer and have been a major factor in the growth of home infusion.
Syringes and Needles
 The basic parts of a syringe are the barrel, plunger, and tip. The barrel is a tube that is open at one end and tapers into a hollow tip at the other end. The plunger is a piston-type rod with a slightly cone-shaped top that passes inside the barrel of the syringe. The tip of the syringe provides the point of attachment for a needle. The volume of solution inside a syringe is indicated by graduation lines on the barrel. Graduation lines may be in milliliters or fractions of a milliliter, depending on the capacity of the syringe. The larger the capacity, the larger the interval between graduation lines.
The basic parts of a syringe are the barrel, plunger, and tip. The barrel is a tube that is open at one end and tapers into a hollow tip at the other end. The plunger is a piston-type rod with a slightly cone-shaped top that passes inside the barrel of the syringe. The tip of the syringe provides the point of attachment for a needle. The volume of solution inside a syringe is indicated by graduation lines on the barrel. Graduation lines may be in milliliters or fractions of a milliliter, depending on the capacity of the syringe. The larger the capacity, the larger the interval between graduation lines.
There are three common types of syringe tips: Slip-Tip®, Luer-Lok®, and eccentric. Slip-Tips® allow the needle to be held on the syringe by friction. The needle is reasonably secure, but it may come off if not properly attached or if considerable pressure is used. Luer-Lok® tips incorporate a collar with grooves that lock the needle in place. Eccentric tips, which are off-center, are used when the needle must be parallel to the plane of injection such as in an intradermal injection.
Syringes come is different sizes ranging from 1 to 60 ml. As a rule, select a syringe whose capacity is the next size larger than the volume to be measured. For example, a 3 ml syringe should be selected to measure 2.3 ml, or a 5 ml syringe to measure 3.8 ml. In this way, the graduation marks on the syringe will be in the smallest possible increments for the volume measured. Syringes should not be filled to capacity because the plunger can be easily dislodged.
The Cornwall syringe is used when many repetitions of filling a syringe to the same volume is needed. It is a manual device that has a two-way valve that attaches to both the syringe and the solution to be drawn into the syringe. Each time the grip is released, the syringe fills with solution. Each time the grip is compressed, the syringe volume is expelled. There are electronic versions of this basic design concept.
Needles
 A needle has three parts, the hub, the shaft, and the bevel. The hub is at one end of the needle and is the part that attaches to the syringe. The shaft is the long slender stem of the needle that is beveled at one end to form a point. The hollow bore of the needle shaft is known as the lumen. Disposable needles should always be used when preparing admixtures as they are presterilized and individually wrapped to maintain sterility.
A needle has three parts, the hub, the shaft, and the bevel. The hub is at one end of the needle and is the part that attaches to the syringe. The shaft is the long slender stem of the needle that is beveled at one end to form a point. The hollow bore of the needle shaft is known as the lumen. Disposable needles should always be used when preparing admixtures as they are presterilized and individually wrapped to maintain sterility.
 Needle size is designated by length and gauge. The length of a needle is measured in inches from the juncture of the hub and the shaft to the tip of the point. Needle lengths range from 3/8 inch to 3 1/2 inches; some special use needles are even longer. The gauge of a needle, used to designate the size of the lumen, ranges from 27 (the finest) to 13 (the largest).
Needle size is designated by length and gauge. The length of a needle is measured in inches from the juncture of the hub and the shaft to the tip of the point. Needle lengths range from 3/8 inch to 3 1/2 inches; some special use needles are even longer. The gauge of a needle, used to designate the size of the lumen, ranges from 27 (the finest) to 13 (the largest).
There are two considerations when choosing a needle size; the viscosity of the solution, and the nature of the rubber closure on the parenteral container. Needles with larger lumens should be used for viscous solutions. Smaller gauge needles are preferred if the rubber closure can be cored easily. Coring is when a needle punctures or tears a piece of the rubber closure and the piece then falls into the container and creates particulate material contamination.
Vascular Access Needle Gauge Recommendations
|
Gauge |
Appropriate Use |
Comments |
|
16-18 |
IV infusion: |
Large vessel required |
|
19-20 |
IV infusion: |
Large vessel required |
|
21 |
IV injection or infusion |
|
|
22-23 |
IV infusion |
Suitable for small or fragile veins |
|
24-27 |
IV infusion |
Especially useful for very small veins |